References: 1.
Jarius S, Ruprecht K, Wildemann B, et al. Contrasting disease patterns in seropositive and seronegative neuromyelitis optica: a multicentre study of 175 patients.
J Neuroinflammation.
2012;9:14.
2.
Mealy MA, Mossburg SE, Kim SH, et al. Long-term disability in neuromyelitis optica spectrum disorder with a history of myelitis is associated with age at onset, delay in diagnosis/preventive treatment, MRI lesion length and presence of symptomatic brain lesions.
Mult Scler Relat Disord.
2019;28:64-68.
3.
Kim SM, Kim SJ, Lee HJ, Kuroda H, Palace J, Fujihara K. Differential diagnosis of neuromyelitis optica spectrum disorders.
Ther Adv Neurol Disord.
2017;10(7):265-289.
4.
Hamid SHM, Whittam D, Mutch K, et al. What proportion of AQP4-IgG-negative NMO spectrum disorder patients are MOG-IgG positive? A cross sectional study of 132 patients.
J Neurol.
2017;264(10):2088-2094.
5.
Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica.
Lancet Neurol.
2007;6(9):805-815.
6.
Hinson SR, Lennon VA, Pittock SJ. Autoimmune AQP4 channelopathies and neuromyelitis optica spectrum disorders.
Handb Clin Neurol.
2016;133:377-403.
7.
Pereira WL, Reiche EMV, Kallaur AP, Kaimen-Maciel DR. Epidemiological, clinical, and immunological characteristics of neuromyelitis optica: a review.
J Neurol Sci.
2015;355(1-2):7-17.
8.
Mutch K, Methley A, Moore P, Jacob A. Life on hold: the experience of living with neuromyelitis optica.
Disabil Rehabil.
2014;36(13):1100-1107.
9.
Ghasemi N, Razavi S, Nikzad E. Multiple sclerosis: pathogenesis, symptoms, diagnoses and cell-based therapy.
Cell J.
2017;19(1):1-10.
10.
Kawachi I, Lassmann H. Neurodegeneration in multiple sclerosis and neuromyelitis optica.
J Neurol Neurosurg Psychiatry.
2017;88(2):137-145.
11.
Masuda H, Mori M, Uzawa A, et al. Recovery from optic neuritis attack in neuromyelitis optica spectrum disorder and multiple sclerosis.
J Neurol Sci.
2016;367:375-379.
12.
Bukhari W, Prain KM, Waters P, et al. Incidence and prevalence of NMOSD in Australia and New Zealand.
J Neurol Neurosurg Psychiatry.
2017;88(8):632-638.
13.
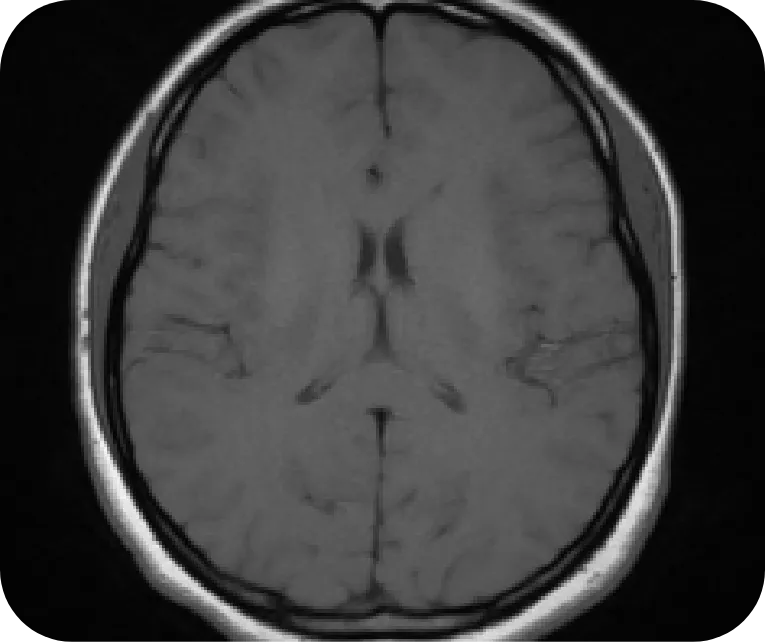
Gaillard F. Normal brain (MRI). Radiopaedia. Published July 2, 2015. Accessed July 26, 2022. https://radiopaedia.org/cases/normal-brain-mri-6?lang=us
14.
Dutra BG, da Rocha AJ, Nunes RH, Maia ACM Jr. Neuromyelitis optica spectrum disorders: spectrum of MR imaging findings and their differential diagnosis.
Radiographics.
2018;38(1):169-193.
15.
Di Muzio B. Normal cervical spine MRI. Radiopaedia. Published July 19, 2015. Accessed July 26, 2022. https://radiopaedia.org/cases/normal-cervical-spine-mri-1?lang
16.
Trebst C, Jarius S, Berthele A, et al. Update on the diagnosis and treatment of neuromyelitis optica: recommendations of the Neuromyelitis Optica Study Group (NEMOS).
J Neurol.
2014;261(1):1-16.
17.
Kitley J, Leite MI, Nakashima I, et al. Prognostic factors and disease course in aquaporin-4 antibody-positive patients with neuromyelitis optica spectrum disorder from the United Kingdom and Japan.
Brain.
2012;135(pt 6):1834-1849.